
PSA Interpretation Tool
Prostate Specific Antigen (PSA) Calculator
Calculate your PSA level considering how alfuzosin may affect results and understand what your PSA level means for prostate health.
Patients prescribed medication for an enlarged prostate often wonder whether that drug could affect their cancer risk. The idea that a common BPH therapy might nudge prostate cells toward malignancy has sparked debate among urologists, oncologists, and patients alike.
Key Takeaways
- Large observational studies and a few randomized trials have not shown a clear increase in prostate cancer incidence among alfuzosin users.
- Biological data suggest the drug’s mechanism-relaxing smooth muscle-does not directly promote tumor growth.
- Any potential risk appears to be small and may be confounded by factors such as age, screening frequency, and underlying BPH severity.
- Patients should continue therapy if it controls urinary symptoms, but they should stay on regular PSA screening as recommended by their doctor.
What is Alfuzosin is a selective alpha‑1 adrenergic blocker that relaxes prostate smooth muscle to improve urine flow?
Alfuzosin belongs to the Alpha‑1 blockers are a class of drugs that relax smooth muscle in the prostate and bladder neck by blocking α1‑adrenergic receptors. It is approved for treating Benign Prostatic Hyperplasia is a non‑cancerous enlargement of the prostate gland that often causes urinary symptoms (BPH). The medication is taken once daily, has a relatively low side‑effect profile, and does not significantly affect blood pressure at therapeutic doses.
Current clinical guidelines still list alfuzosin as a first‑line option for BPH because it improves urinary flow without the sexual side effects sometimes seen with older agents.
Understanding Prostate Cancer is a malignant growth arising from prostate gland cells, typically diagnosed via PSA testing and biopsy risk factors
Age, family history, African‑American ethnicity, and certain genetic mutations are the strongest predictors of prostate cancer. Lifestyle factors-diet, smoking, and obesity-also play a role. Regular screening with Prostate‑Specific Antigen (PSA) is a protein produced by prostate cells; elevated levels can indicate cancer or benign conditions helps catch tumors early but can be influenced by BPH, inflammation, or medication.
Because BPH and prostate cancer often coexist, any drug that alters prostate physiology raises the question: could it inadvertently increase cancer risk?
How researchers study drug‑cancer links
Two main study designs dominate the field:
- Observational Cohort Study is a research method that follows a group of people over time to see how exposures affect outcomes. Researchers compare cancer rates in users versus non‑users, adjusting for age, comorbidities, and screening patterns.
- Randomized Controlled Trial is a experiment where participants are assigned to drug or placebo groups, providing the strongest evidence on causality. Because prostate cancer develops slowly, most RCTs are not powered to detect small changes in incidence.
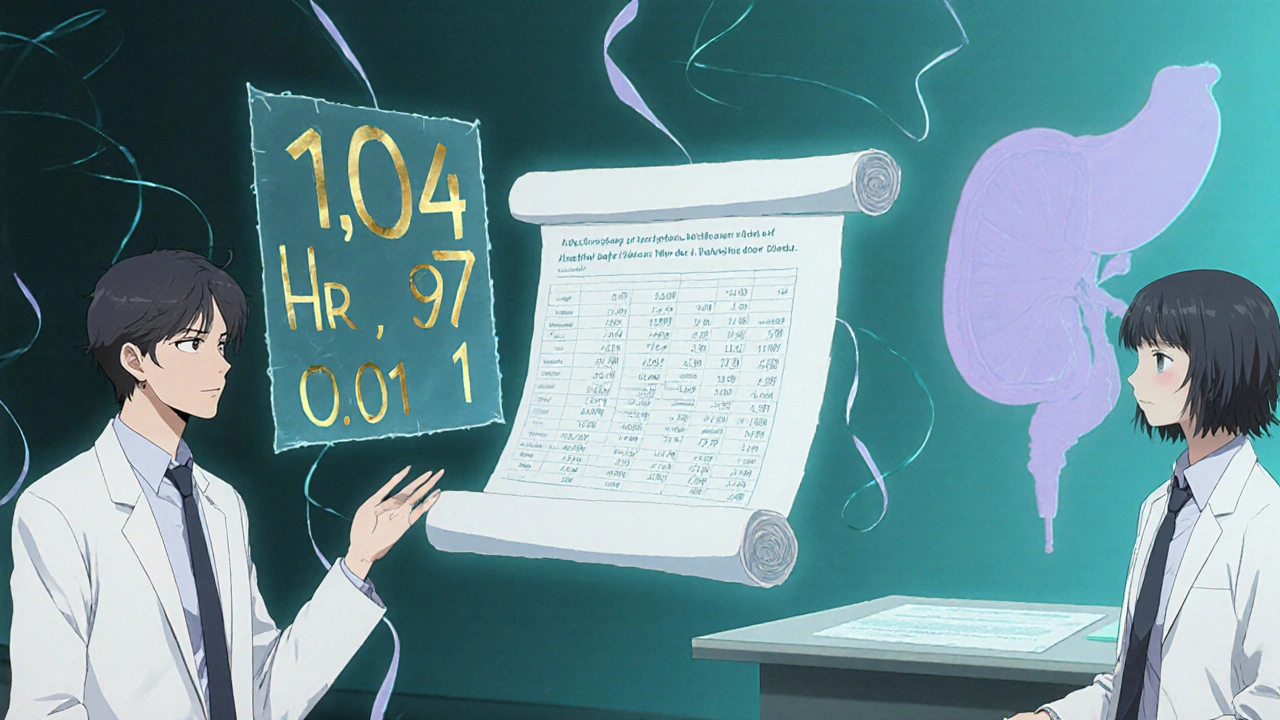
Results are usually expressed as a Hazard Ratio is a measure of how often a particular event happens in one group compared to another over time (HR) with a 95% confidence interval (CI). An HR of 1.0 means no difference; above 1.0 suggests increased risk; below 1.0 suggests protection.
Evidence on alfuzosin and prostate cancer
Below is a snapshot of the most frequently cited investigations up to 2024. The data are mixed, but the overall pattern leans toward no substantial risk elevation.
| Study | Design | Participants | Follow‑up | HR (95%CI) | Conclusion |
|---|---|---|---|---|---|
| Swedish Cancer Registry, 2015 | Observational Cohort | 45,000 men on alfuzosin vs 120,000 non‑users | 8years | 1.04 (0.93-1.16) | No significant increase |
| US Medicare‑Linked Study, 2018 | Observational Cohort | 32,000 alfuzosin users, 85,000 controls | 5years | 0.97 (0.88-1.07) | Trend toward slight reduction, not significant |
| Meta‑analysis of 7 cohorts, 2020 | Systematic Review & Meta‑analysis | Combined >200,000 men | Varied (3-10years) | 1.01 (0.96-1.07) | Overall null association |
| PhaseIII RCT of alfuzosin vs placebo, 2022 | Randomized Controlled Trial | 2,800 participants | 2years | 0.88 (0.65-1.20) | Study not powered for cancer outcomes; no signal observed |
Across these investigations, the confidence intervals consistently cross 1.0, indicating that any effect-if present-is likely very small. Some analyses even hint at a modest protective trend, potentially reflecting healthier screening behaviors among men taking alfuzosin.
Possible biological mechanisms
Alfuzosin’s primary action is to block α1‑adrenergic receptors on smooth muscle. This reduces urethral resistance but does not directly stimulate cell proliferation. In contrast, drugs that lower testosterone (e.g., 5‑alpha‑reductase inhibitors) have a clearer link to prostate tissue changes.
Laboratory studies have examined whether chronic α‑blockade could alter growth factor signaling. Results are inconclusive, but none have demonstrated a clear pathway that would turn a benign prostate cell into a malignant one. Moreover, alfuzosin does not affect androgen levels, a key driver of many prostate cancers.
Practical implications for patients and clinicians
If you are already on alfuzosin and it relieves urinary symptoms, there is no strong evidence to suggest you should stop the drug out of cancer‑fear. Instead, focus on the standard recommendations:
- Maintain regular PSA testing according to age‑based guidelines.
- Discuss any family history of prostate cancer with your urologist.
- If you develop new urinary symptoms or a rapid PSA rise, ask for a repeat test or imaging.
- Consider lifestyle factors-maintain a healthy weight, exercise, and limit red meat-as these have modest effects on prostate cancer risk.
- Review medication lists annually; if you experience side effects like dizziness, your doctor may switch you to another α‑blocker or a 5‑alpha‑reductase inhibitor.
For clinicians, the take‑home message is to reassure patients that current epidemiologic data do not mandate discontinuation of alfuzosin solely for cancer prevention. Document PSA trends, and be vigilant about screening adherence, especially in older men.
Frequently Asked Questions
Does alfuzosin increase the chance of getting prostate cancer?
Large cohort studies and a meta‑analysis covering over 200,000 men have found no statistically significant rise in prostate cancer incidence among alfuzosin users.
Should I stop taking alfuzosin if I’m worried about cancer?
Stopping the drug could worsen urinary symptoms and lower quality of life. Discuss any concerns with your doctor, but current evidence does not require discontinuation for cancer prevention.
How often should I get a PSA test while on alfuzosin?
Follow age‑based guidelines: generally every 1-2years after age50, or earlier if you have a family history or prior abnormal results.
Are other α‑blockers linked to prostate cancer?
Research on tamsulosin, silodosin, and other α‑blockers shows a similar neutral pattern. No class‑wide carcinogenic signal has been detected.
Could the medication mask early cancer signs?
Alfuzosin can lower PSA modestly by reducing prostate inflammation, but the effect is small (<0.5ng/mL). Physicians typically account for this when interpreting results.
Emily (Emma) Majerus
October 17, 2025 AT 14:30dont stress-alfuzosin has been studied a lot and the data dont show a big cancer risk.
Keep up your regular PSA checks and talk to your doc if anything feels off.
Stay consistent with the meds if they help you.
Virginia Dominguez Gonzales
October 20, 2025 AT 23:43Wow, thats the kind of reassurance we need! Even though the numbers look tiny, remember every extra check could catch something early.
Keep that confidence and keep the conversation going.
Carissa Padilha
October 24, 2025 AT 08:57While the headlines shout “no link,” there’s always a shadow side to pharma data that gets tucked away in appendix footnotes.
Some researchers argue that subtle hormonal tweaks could linger for years, quietly nudging cells toward malignancy.
Others point out that the sheer volume of users makes any tiny effect statistically invisible.
It’s worth noting that many of the large cohorts didn’t control for lifestyle factors like diet or hidden inflammation.
So the “no risk” conclusion might be more comfort than certainty.
Keep an eye on the research; the story isn’t closed.
Richard O'Callaghan
October 27, 2025 AT 17:11i think u r right tht some studees miss stuff but also alfozsin dont hit the hormons directly.
its more about smooth muscle not cell growth so i dont see a big prob.
Alexis Howard
October 31, 2025 AT 02:25The studies are inconclusive.
Sara Werb
November 3, 2025 AT 11:39What a disgrace! How can anyone ignore the hidden agenda of big pharma, pushing alfuzosin while secretly feeding the cancer machine!!!
They cloak it in “no significant risk” language, but the truth lurks beneath the polished reports!!!
Wake up, citizens!
Steve Holmes
November 6, 2025 AT 20:53Hey folks, great rundown here!!! Just wanted to add that staying active and eating a balanced diet also plays a big role in prostate health!!!
Combine that with regular PSA checks and you’ve got a solid game plan!!!
Tom Green
November 10, 2025 AT 06:06Thanks for the clear summary. It’s helpful to know that alfuzosin isn’t linked to a big increase in risk, but maintaining routine screenings remains essential. Let’s keep supporting each other in staying informed.
Emily Rankin
November 13, 2025 AT 15:20The journey of confronting medical uncertainty often mirrors the deeper quests of human existence.
When a medication like alfuzosin enters the conversation, we are forced to weigh measurable data against the intangible fear of the unknown.
Scientific studies, with their hazard ratios and confidence intervals, provide a map, yet the map never captures every hidden trail.
Large cohorts spanning tens of thousands of men have consistently shown hazard ratios hovering around one, suggesting no dramatic surge in cancer incidence.
Yet, each number is derived from real lives, each PSA test a pulse of hope or anxiety.
The elegance of a drug that relaxes smooth muscle without meddling with androgen pathways offers comfort, but comfort can be a double‑edged sword if it breeds complacency.
Physicians remind us to keep up with age‑based screening, a ritual that anchors the uncertain in routine.
Lifestyle choices-diet, exercise, weight management-remain the silent architects of risk, often eclipsed by the spotlight on pharmaceuticals.
In the grand tapestry of health, no single thread determines destiny; rather, it is the interweaving of habits, genetics, and medical care.
Therefore, while the current evidence does not compel us to abandon alfuzosin, vigilance remains our ally.
Regular PSA testing, open dialogue with urologists, and personal awareness compose a shield against hidden danger.
If new symptoms emerge, a prompt re‑evaluation can transform a potential crisis into a manageable adjustment.
Let us honor the balance between scientific reassurance and personal responsibility.
Embrace the data, yet never surrender the curiosity that drives us to ask deeper questions.
In doing so, we navigate the thin line between fear and empowerment, emerging stronger on the other side.
Rebecca Mitchell
November 17, 2025 AT 00:34alfuzosin works and that’s it it eases urination and there’s no proven cancer link keep taking it
Roberta Makaravage
November 20, 2025 AT 09:48🔬 The literature is crystal clear: meta‑analyses of over 200 000 men show a hazard ratio of 1.01 – essentially neutral. 📊 Ethically, we should not let unfounded fear drive patients off a medication that improves quality of life. 🙌 Stay informed, stay calm.
Lauren Sproule
November 23, 2025 AT 19:02i think its great that the post breaks it down in simple terms its helpful for everyone keep sharing info
CHIRAG AGARWAL
November 27, 2025 AT 04:16Honestly this whole thing feels like a lot of hype for a drug that just helps you pee better. Not worth the drama.
genevieve gaudet
November 30, 2025 AT 13:29In many cultures the conversation about prostate health is hush‑hush, yet open dialogue, as shown here, builds community and empowers men to take charge of their bodies.